Cryoglobulins
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
CRYOGLOBULINS
Cryoglobulinemia: definition
· Defined as the presence of serum (or plasma) proteins (Ig) that precipitate at low temperatures and "solubilize" upon rewarming at 37°C
· The incidence increases after the age of 60
· They are classified according to Ig characteristics

CRYOGLOBULINS
· Crioglobulins are an artificially induced laboratory phenomenon.
· Serum proteins reversibly precipitate or "gelify" at temperatures below 37°C, even at low concentrations (less than 0,1mg/dL).
· From the very first observations, it has been shown that cryoglobulins are mainly composed of immunoglobulins.

The History of Cryoglobulins
The first clinical observation of this phenomenon dates back to 1933, when Wintrobe and Buell first observed cryoprecipitates in a patient affected by multiple myeloma.
The History of Cryoglobulins
· Further reports of this phenomenon continued over several years, always associated with cases of multiple myeloma or lymphoproliferative diseases. Cryoglobulins were thus confined to hematological areas of interest.
· In 1947 Lerner and Watson demonstrated the reversibility of this phenomenon, providing a definition of "cryoglobulins" and reporting their presence in patients affected by a variety of diseases.
The History of Cryoglobulins
In 1966 Metzler and Franklin described the presence of mixed cryoglobulinemia in 29 cases. Of these, 12 had both IgM and IgG immunoglobulins, where IgM had Rheumatoid Factor activity (FR).
Among all cases of mixed cryoglobulinemia, 9 presented symptoms of purpura, asthenia and arthralgia, whereas 4 were affected by renal failure.
The History of Cryoglobulins
In 1974 Brouet and his collaborators electrophoretically characterized three distinctive immunochemical cryoglobulin patterns, classified as follows:
Type I - monoclonal Ig component
Type II - polyclonal Ig component + monoclonal Ig component
Type III - Two or even three polyclonal Ig components

Summary
1) The first clinical observation of the phenomenon dates back to 1933, when Wintrobe and Buell reported this finding in a patient affected by multiple myeloma.
2) In 1947, Lerner and Watson proved that the phenomenon was reversible. For the first time, cryoglobulins were defined and their presence was reported in patients affected by different diseases.
3) In 1966, Metzler and Franklin defined mixed cryoglobulinemia in a case study. Out of 29 cases, 12 had IgM and IgG cryoglobulinemia, where IgM showed rheumatoid factor (RF) activity.
4) In 1974, Brouet et al. classified cryoglobulins according to the following criteria:
Type I - Monoclonal Ig components
Type II - Polyclonal Ig component + Monoclonal Ig component
Type III - Two or even three polyclonal Ig components.
CLASSIFICATION 2
1) Musset L, Diemert MC, Taibi F, et al. Characterization of cryoglobulins by immunoblotting. Clin Chem 1992; 38: 798-802.
2) Tissot JD, Schifferli JA, Hochstresser DF et al. Two-dimensional polyacrylamide gel electrophoresis analysis of cryoglobulins and identification of an IgM - associated peptide. J Immunol Meth 1994; 173: 63-75.
The New Classification by Pontet.
Subdivides Type II cryoglobulinemia into two groups:
· IIa: presence of a monoclonal Ig + polyclonal Igs
· IIb: presence of several monoclonal Igs + polyclonal Igs

Pontet F, Halimi C, Brocarde A. and Delacour T. Biclonal immunoglobuin M dysglobulinaemia: evolving aspects in a case of primary Sjogren syndrome. Eur J Clin Chem Clin Biochem 1997: 35 (4): 287-90
A new classification on the basis of immunochemical patterns
· Type I: they consist of monoclonal immunoglobulins.
· Type III: Mixed polyclonal cryoglobulins. They customarily consist of polyclonal IgM with anti-IgG activity (rheumatoid factor) and are associated with circulating immunocomplexes. They are often found in hepatitis C.
· Type IIa: Mixed cryoglobulins with a monoclonal component and polyclonal Ig. They consist of immunoglobulins that belong to two different classes, one of which is monoclonal. Monoclonal IgM cryoglobulins and polyclonal IgG cryoglobulins are the most common. IgM thus has a rheumatoid factor activity by reacting with the Fc fragment of the IgG.
· Type IIb: Mixed cryoglobulins consisting of oligoclonal Ig and polyclonal Ig. Although this profile is predominantly seen among patients affected by hepatitis C virus, it may also occur following kidney transplants, in non-Hodgkin’s lymphoma, and in AIDS. It may involve an intermediate state that can evolve toward Type III or Type IIa;
Le Carrer D, Cryoglobulinemies: proposition d’un protocole d’exploration biologique. Actualisation de leur classification – Feuillets biol. 39/221,62, 1998
Which taxonomic classification should be adopted?
Should the classification be updated in a “convulsive” fashion according to the new immunochemical patterns?
1) the classification becomes difficult to interpret, and only available to "few" connaisseurs.
2) communication difficulties between clinicians and laboratory staff
Should one rely on Brouet's
classification?
Integrating new immunochemical patterns within the three classes, according to clinical manifestations common to both old and new inspective patterns

New Classification: modified Brouet's
TYPE I
Monoclonal Igs
TYPE II
One or more monoclonal Igs + polyclonal Igs
TYPE III
Two or more polyclonal Igs
Two or more oligoclonal Ig bands.
Passerini G.,Basile U. Biochim Clin 2010 N°3 218-222
Cryoglobulinemia: classification
Three cryoglobulin subgroups can be distinguished, in association with a wide range of diseases including haematological, autoimmune, infectious and chronic affections (in particular with the Hepatitis "C" virus).

TYPE I CRYOGLOBULINEMIA
- Type I Cryoglobulinemia is the least common among Cryoglobulinemias (comprising 5-10% of all cases). It mainly consists of monoclonal Igs (usually IgMs or IgGs) which rarely show rheumatoid factor (RF) activity (ie, antibody activity towards other immunoglobulins)
- It is typically observed among patients affected by Multiple Myeloma, Waldestroem's disease, MGUS and lymphoproliferative disorders.

TYPE II and TYPE III MIXED CRYOGLOBULINEMIA
· Accounts for over 80% of all cryoglobulinemias
· So called as it consists of two different immunoglobulins
· Appears in the context of infectious or autoimmune diseases, or as a separate entity without any association with obvious causal factors (Essential Mixed Cryoglobulinemia, EMC)
· Given the detection of HCV in 90% of patients with EMC, however, this term is no longer considered appropriate
Cryoprecipitation: intrinsic factors
· Structural changes in the variable portion of the Ig heavy and light chains.
· Reduced concentration of sialic acid and glucosamine residues.
· Reduced concentration of galactose in the Fc portion of Igs, responsible for non-specific Fc-Fc interactions.
Cryoprecipitation: intrinsic factors
· Conformational changes of Igs as a result of temperature variations, implying lower polarity and decreased solubility.
· Increased protein concentration favouring aggregation.
· Optimal pH for precipitation: approaching the isoelectric point (5.5-8).
· Ionic strength and presence of calcium, barium and manganese.
Cryoglobulinemia: the phenomenon of cryoprecipitation
· The mechanisms of cryoprecipitation are poorly understood.
· In type I cryoglobulinemia, the cryoprecipitation process seems to be an intrinsic characteristic of monoclonal immunoglobulins. It is strictly related to the integrity of their quaternary structure, since Fc and Fab fragments usually lose their precipitability at low temperatures upon separation.
· The cryoprecipitation process could be triggered by changes in the amino acid composition, as well as by variations in the carbohydrate content of immunoglobulin heavy and light chains. As a result of the overall increase in hydrophobicity, the molecules thereby lose their solubility.
Cryoglobulinemia: the cryoprecipitation phenomenon
- The mechanisms of cryoprecipitation have yet to be fully clarified.
In type II and III cryoglobulinemia:
- Cryoprecipitation is mainly due to interactions occurring between immunoglobulins, rather than to characteristics of the individual immunoglobulin components.
- In IgG-IgM mixed cryoglobulinemia, the anti-IgG IgM component specifically determines cryoprecipitation.

Mixed cryoglobulinemia:
the immunocomplex disease
- Mixed cryoglobulinemia (MC) is characterized by the presence of immunocomplexes, where IgGs or IgMs behave as antigens, and IgMs or either mono- or polyclonal IgG3 behave as antibodies, with RF (anti-Ig) activities.
- This may induce the development of an immune complex disease. This condition is histologically characterized by inflammatory lesions affecting involved vessels, as well as immune deposits in target organs showing the same composition of serum cryoprecipitate.
Models of structural transition
Aggregation
Network
Sol/Gel

EPIDEMIOLOGY
Rare disease? Probably NOT
The true prevalence is unknown:
· Inadequate epidemiological studies
· Due to the absence or non-specific clinical manifestations, as well as to the multi-specialized area of interest required by the underlying disease.
rheumatologist
neurologist
dermatologist
hepatologist
clinical pathologist
nephrologist
A POSSIBLE APPROACH TO THE CLASSIFICATION
OF THE CRYOGLOBULINEMIC SYNDROME
· cryocrit > 1% for at least 6 months
two of the following symptoms: purpura, fatigue, arthralgia
C4 < 8 mg%
Positive RF test in serum (must be distinguished whether mono- or polyclonal)
· Secondary if it occurs in association with: connective tissue disease, chronic liver disease, lymphoproliferative disorders and/or infections. In the absence of any one of the previously mentioned conditions, it should be defined as seemingly essential.
· Evaluation of the extension of the vasculitic process: hepatic involvement, renal affections, peripheral neuropathies
· Identification of microlymphoma-like nodules in bone marrow biopsies.
· The cryoglobulinemic components may be seen as deposits within cutaneous and renal vasculitic lesions. The exact causes of these deposits, as well as the underlying causes of vascular damage, have yet to be determined.
Etiopathogenesis: food for thought
Mixed cryoglobulinemia has been classified among systemic vasculitis (histopathological pattern: Leukocytoclastic vasculitis), within the subgroup of small vessels vasculitis (involving arterioles, capillaries and venules) as well as cutaneous leukocytoclastic vasculitis and Henoch-Schonlein purpura
(Meltzer M, Franklin EC, et al. Am J Med 1966)
Etiopathogenesis: food for thought
- Clinicopathological observations concerning the cryoglobulinemic syndrome
- High prevalence of liver disease
- Discovery of the hepatitis C virus (HCV) in 1989
- Association with organ- and non-organ-specific autoimmune diseases
- Association with lymphoproliferative disorders + malignant neoplasms

Etiopathogenesis: food for thought
1. Discovery of HCV as the main causative agent of ‘nonA/nonB hepatitis’. The detection of
anti-HCV antibodies, by means of first generation kits, showed 30-50% positivity among patients affected by cryoglobulinemic syndromes.
2. HCV infection was definitely ascertained in 86% of 42 subjects affected by MC (HCV RNA detected by PCR techniques) (Ferri C et al, Association between hepatitis C virus and mixed cryoglobulinemia. Clin Exp Rheumatol 1991)
3. Following the discovery of the close association between MC and HCV, as well as the
biological characteristics of HCV, such as its hepato- and lymphotropism (Zignego AL et al. J Hepatol 1992) it was possible to formulate the following hypotheses concerning pathogenicity:
- Cryoglobulinemia as a model of circulating immune complex-induced (CIC) systemic vasculitis;
- Cryoglobulinemia as clinical expression of an underlying 'benign' lymphoproliferative process;
- Hepatitis C virus as disease determinant, as it is involved in both CIC generation (Agnello V. et al. N Engl J Med 1992) as well as in the initiation of B-lymphocyte proliferation.
Etiopathogenesis: food for thought
Cryoglobulin production as a result of chronic stimulation of the immune system by the C virus.
I. Interactions between the E2 protein of the virus and CD81 on lymphocytes
II. CD81 is a surface protein found on B cells. It forms complexes with other molecules (such as CD21 - CD19 - Leu13)
III. Amplification of the physiological polyclonal stimulation of the B cell compartment induced by HCV infection
IV. t (14; 18) translocations and/or rearrangements of bcl2 have been reported in a significant number of HCV-infected cases, thus inhibiting apoptosis and prolonging cell survival...
Etiopathogenesis: food for thought
HCV is a hepatotropic and lymphotropic virus, which can exert an oncogenic effect in two different directions: by inducing hepatocellular carcinoma and B-cell lymphoma
Cryoglobulins and HCV
- HCV-related cryoglobulinemias are correlated with the clinical manifestations that Meltzer and Franklin spotted in the triad composed of purpura, arthralgia and fatigue. Nevertheless, other organs and systems may be involved to varying degrees.
- Correlation with HCV-Ab (higher prevalence in association with type II).
- The virus is pathogenetically involved, as viral RNA has been recovered in the cryoprecipitate.
Ferri C et al. REVIEW Cryoglobulins. Journal of Clinical Pathology 2002;55:4-13

Extrahepatic manifestations of hepatitis
CLASSIFICATION CRITERIA
Diagnostic certainty: 3 major criteria or one major serological criterion + 2 minor clinical criteria and + 2 minor histological / serological criteria
Diagnostic probability:
- 1 major serological criterion + 1 minor clinical criterion + 1 serological or histological criterion
- Purpura or Leucoclastic vasculitis + 1 minor clinical criterion +1 minor serological or histological criterion
- 2 minor clinical criteria + 2 minor serological or histological criteria
Clinical Manifestations
· Clinical manifestations associated with HCV infection are often inconstant
· Approximately 50% of monoclonal cryoglobulinemias and 15% of mixed cryoglobulinemias are asymptomatic.
The most common symptoms of monoclonal cryoglobulinemias include:
Raynaud's phenomenon (40%)
Acrocyanosis (15%)
Vascular purpura (15%)
Cold urticaria (15%)
Ulcers supra malleolar and livedo reticularis (1%)
Triad: Purpura - Asthenia - Arthralgia

Cryoglobulin detection
This is a simple test, although several aspects can complicate it:
- Preanalitical aspects
- Aspects concerning quantification and characterization
Critical Preanalytical Aspects
Serum volume
Critical Analytical Aspects
Observation time
Cryocrit measurement standardization
Critical Postanalytical Aspects
Taxonomic reference
Is cryoglobulin detection requested in the appropriate manner?
Generally, this test is requested in the appropriate contexts, although it is often ignored in clinical settings where it may be performed to aid in the diagnosis or prognosis of diseases.
When should cryoglobulin detection be requested?
1. Patients with monoclonal components
2. Patients affected by Raynaud's syndrome, as well as in subjects presenting with intolerance/pain of the extremities at low temperatures
3. Symptomatic subjects affected by Meltzer's triad
4. Presence of systemic vasculitis, lymphoproliferative disorders, autoimmune diseases, viral (HCV) infections
When should cryoglobulin detection be requested?
1. Purpura, urticaria, ulcers
2. Renal failure, neuropathies
3. In the presence of decreased C4 levels and increased RF levels
4. Abnormal laboratory tests, suggestive of interferences
5. Occasional cryoglobulin detection
Interference by cryoglobulins with other laboratory tests
The presence of cryoglobulins in serum may create a clinical challenge for the interpretation of several laboratory tests
· BLOOD COUNT
· ESR
· SERUM PROTEIN ELECTROPHORESIS
· HCV DIAGNOSTICS (Ab and RNA)
LABORATORY INVESTIGATIONS
Laboratory request appropriateness
Cryoglobulin testing should only be performed in patients with clinical or laboratory evidence suggestive of associated diseases
Kallemuchikkal & Gorevic, Arch Pathol Lab Med 1999, 123:119-25
Keren et al, Guidelines for Monoclonal Gammopathies - Guideline 8 - Arch Pathol Lab Med 1999, 123:106-7
PREANALYTICAL PHASE
Phlebotomy
Preparation - Test tubes - Temperature - Volume
Transport
Temperature - Coagulation - Centrifugation - Preservatives
ANALYTICAL PHASE
Incubation
Serum volume - Temperature - Time
Quantification
CRG measurement - Check at 37°C - Other determinations
Characterization
Washes - Typing
POSTANALYTICAL PHASE
Reporting
Detection - Classification - Reference values
CRYOGLOBULIN DETECTION
Blood collection procedure
· At least 10 mL of blood. Samples must be immediately stored at 37 °C
· Allow blood to clot at 37 °C for at least 30 '
· Centrifuge at 2500 rpm for 10 ' at 37 °C
· Separate serum immediately. Place in Wintrobe tubes and incubate at 4 °C
Kallemuchikkal & Gorevic, Arch Pathol Lab Med 1999, 123:119-25
Keren et al, Guidelines for Monoclonal Gammopathies - Guideline 8 - Arch Pathol Lab Med 1999, 123:106-7
Blood collection procedure
· Serum cryoglobulin detection requires strict adhesion to protocol procedures recommending the use of pre-heated material (in water bath at 37 °C) for both blood collection and transport to the laboratory.
· The use of test tubes with separator gel is not recommended due to the risk of possible release of interfering substances during incubation at 37 °C.
· If tubes without gel barriers are not available, then the provider should be enquired for specific information concerning the characteristics of the gel.
Passerini G.,Basile U. for the SIBIOC protein study group
Detection, quantification and characterization of cryoglobulins: indications for a common protocol
Biochim Clin 2010 N°3 218-22

Evaluation of cryoprecipitate
Incubate at 4°C for at least 7 days
· Observe the presence of eventual flocculate, precipitate or gel
· Verify the reversibility of cryprecipitation
· Exclude the presence of fibrin-fibrinogen complexes or of heparin-fibronectin complexes
Kallemuchikkal & Gorevic, Arch Pathol Lab Med 1999, 123:119-25
Keren et al, Guidelines for Monoclonal Gammopathies - Guideline 8 - Arch Pathol Lab Med 1999, 123:106-7
Quantification of cryoprecipitate
CRYOCRIT – Percentage obtained by calculating the ratio between the volume of cryoprecipitate and the volume of serum after centrifugation at 1700 rpm for 15' at 4°C
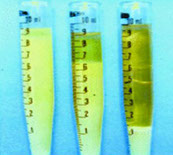
Despite its inaccuracy and poor specificity, clinicians consider it as the 'gold standard' for follow-up.
It is of little use for comparing different patients or for assessing the activity of associated diseases.
Kallemuchikkal & Gorevic, Arch Pathol Lab Med 1999, 123:119-25
Shihabi ZK. Ann Clin Lab Sci 2006;36:395-408
Quantification
TOTAL PROTEINS
Methods
· Spectrophotometric detection at 280 nm
· Colorimetric detection (Folin, Bradford or pyrogallol)
Preparation of cryoprecipitate
3-6 washes with cold PBS or saline buffer solution
CRG resolubilization with NaOH 0.1 mmol/L or acetic acid 0.1 mol/L or by incubation at 37 °C
Poorly standardized methods (normal values ≅20 µg/mL)
Brouet JC, et al. Am J Med 1974.57: 775-88.
Musset L, et al. Clin Chem 1992; 38: 798-802.
Kallemuchikkal & Gorevic, Arch Pathol Lab Med 1999, 123:119-25
Quantification
IgG, IgA, IgM
Quantified by means of nephelometric assay performed on native serum (incubated at 37°C) as well as on serum supernatant after cryoprecipitation
ELECTROPHORESIS
Resuspended cryoprecipitate (at 37°C) is run in order to evaluate any increase in the globulin/albumin ratio compared to native serum.
Kallemuchikkal & Gorevic, Arch Pathol Lab Med 1999, 123:119-25
Rapid screening methods
Spectrophotometry at 350 nm
Serum samples are incubated at 10°C. In this way, it is possible to evaluate the aggregation kinetics of CRGs.
The test only requires a couple of minutes, in contrast to the 7 days required by conventional methods for cryoprecipitation detection.
The procedure still needs validation and is thus currently not applicable to routine analysis.
E. Di Stasio et al. “Analysis of the dynamics of cryoaggregation by light-scattering spectrometry” Clin Chem Lab Med 2003;41:153-58
CRG washes
Two washes do not remove all contaminating serum proteins
Characterization of cryoprecipitate
CRG washes
· Use washing solutions at 4°C (physiological or phosphate buffer or PBS with 3% PEG 6000 )
· Dissolve CRG by agitation
· Centrifuge at 2000 rpm for 15 minutes at 4°C
· Repeat washes at least three times
Brouet JC, et al. Am J Med 1974.57: 775-88
Musset L, et al. Clin Chem 1992; 38: 798-802
Shihabi ZK. Ann Clin Lab Sci 2006;36:395-408
Characterization of cryoprecipitate
CRG solubilization
· Incubate at 37°C until completely solubilized
· Eventually add reducing agents, such as 10% acetylcysteine or 1% β-mercaptoethanol or 1% - dithiothreitol 0.5M
Characterizazion of cryoprecipitate
CRG typing
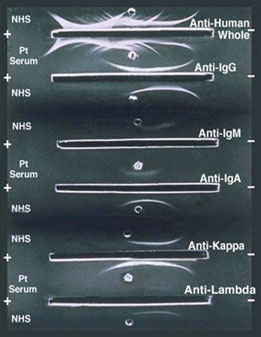
· Immunonofixation on agarose gel (gold standard)
· Immunosubtraction by means of capillary electrophoresis
· Immunoblotting
· 2-dimensional electrophoresis on polyacrylamide gel
IFE is considered the reference technique for qualitative detection of MC in both serum and urine.
It is achieved by combining two types of techniques:
Electrophoresis and immunoprecipitation on solid supports
The operational steps are schematized as follows:
Electrophoretic separation
Immunoprecipitation
Removal of non-precipitated material
Staining
Upon proper execution, IFE considerably amplifies the protein content of a fraction.
Undetectable fractions by electrophoresis are thus rendered visible by staining.
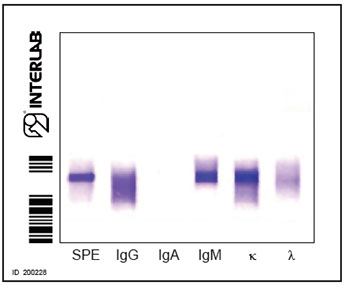
CRG typing
High-resolution agarose gel immunofixation
Type II
IgMκ MC - polyclonal IgGs

Brouet's classification
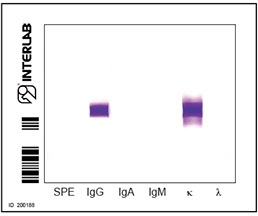
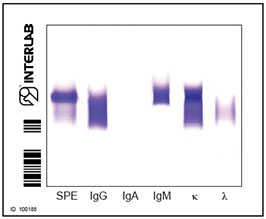
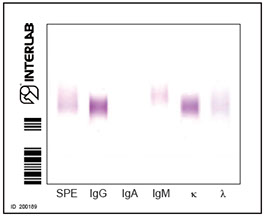
cryocrit=10.0% Type I
CM IgG K
cryocrit=50% Type II
IgMκ MC-polyclonal IgGs
cryocrit <1.0 Type III
Polyclonal IgMs
Microheterogeneous cryoglobulinemias
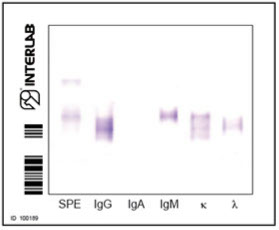
cryocrit <1.0 Type III
oligo/polyclonal IgMs
Reporting
CRYOGLOBULINS
Further investigations
· Complement factors
low or undetectable levels of C3
normal or decreased levels of C4
· Rheumatoid factor
· Anti-HCV antibodies
· Quantitative HCV-RNA analysis
Kallemuchikkal & Gorevic, Arch Pathol Lab Med 1999, 123:119-25
CONCLUSIONS
· Cryoglobulin detection is of considerable relevance
· The test itself is still neglected and misused, as it requires standardization of procedures
· Several issues such as pathogenesis, clinical, therapeutic and laboratory aspects have yet to be clarified
<
>



