Monoclonal Gammopathies of Undetermined Significance
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
MONOCLONAL GAMMOPATHIES
of undetermined significance
MGUS
HISTORICAL PERSPECTIVE
J. Waldenström, 1952: PROTEIN PEAK BY SERUM PROTEIN ELECTRPHORESIS IN THE ABSENCE OF MM, MW AND AL
‘ESSENTIAL HYPERGLOBULINEMIA’
…. IDIOPATHIC
…. ASYMPTOMATIC
…. BENIGN
…. NON-MYELOMATOUS
…. DISCRETE
…. CRYPTOGENIC
…. DISIMMUNOGLOBULINEMIA
‘ IDIOPATHIC PARAPROTEINEMIA’
‘LANTANIC MONOCLONAL GAMMOPATHY’
…. RUDIMENTAL CRYPTOGENIC
…. BENIGN
…. OF UNDETERMINED SIGNIFICANCE (MGUS)
R.A. Kyle, 1978:
Monoclonal gammopathy: definition
· Monoclonal gammopathies are clinical-laboratoristic conditions consisting of a commonly shared feature, implying the clonal proliferation of (more or less mature) B lymphocytes. These cells are capable of synthesizing/secreting immunoglobulins, characterized by identical isotypes and fragments (heavy and light chains)
·The immunoglobulin chain produced consists of a single class as well as the same subclass and idiotype, in other words, the same antigen binding site in the variable region.
MONOCLONAL GAMMOPATHIES
Monoclonal gammopathies thus represent a group of diseases characterized by an excessive production of immunoglobulins by bone marrow plasma cells.
are chronic lymphoproliferative disorders marked by the production of elevated amounts of monoclonal immunoglobulin chains (monoclonal M component) which determine an alteration of electrophoretic profiles of both serum and urine proteins.
"Gammopathy" refers to the fact that most immunoglobulins tend to accumulate within the gamma zone of the protein electrophoretic pattern. The gamma region will thus show a "peak", as a result of the excess immunoglobulins.
The term "monoclonal" indicates that these proteins are all produced by a single plasma cell clone and are all alike, unlike normal polyclonal immunoglobulins.
The following table reports a list of diseases that necessarily imply the presence of MC and those which may occasionally present with MC.
MONOCLONAL COMPONENTS: CHARACTERISTICS AND RECURRENCE
CLINICAL CRITERIA FOR THE DIAGNOSIS OF MGUS
The International Myeloma Working Group: Brit. J. Haematol. 121: 749, 2003
DETECTION OF MCs
Protein electrophoresis enables the detection of monoclonal components upon assessment of the molecular homogeneity of the protein. While the prevalence of the condition in the population does not justify the use of screening tests, the use of EF upon hospital admission of all patients aged 50 and above seems reasonable. The test is also indicated in order to monitor patients undergoing organ transplantation as well as in patients affected by demyelinating peripheral neuropathy.
Graziani MS, Dolci A, Greco C, Luraschi P, Muratore MT, Mussap M, Merlini G for the SIBioC Protein study group. IIndications for the request of serum protein electrophoresis. BC 2008;32:48-51.
ELECTROPHORETIC PATTERNS OF MONOCLONAL GAMMOPATHIES
Serum protein electrophoresis
MONOCLONAL GAMMOPATHY OF UNDETERMINED SIGNIFICANCE (MGUS)
· Incidentally diagnosed during other laboratory investigations
· Absence of clinical features (no symptoms or organ damage)
· Incidence increases with age
· No therapy required
MGUS
Characterized by the presence of monoclonal proteins in serum and/or urine without clinical evidence of either myeloma, Waldenstroem's macroglobulinemia, amyloidosis, lymphoproliferative disorders or other diseases in relationship to the appearance of monoclonal gammopathy.
The term MGUS or essential monoclonal gammopathy appropriately denotes this condition, as opposed to benign monoclonal gammopathy, which falsely connotates a more favorable prognosis. This is in contrast with the clinical evidence showing possible evolution towards overt lymphoplasmocytic forms of the disease, as well as of MGUS as an early stage multiple myeloma.
Incidence
Over 50 years of age: 3.2% incidence
50-59: 1.7 %
>70; 5.3%
More common among males and African-Americans
The risk of progression towards multiple myeloma: 1% / year
Independent of age
Dependent on prognostic factors
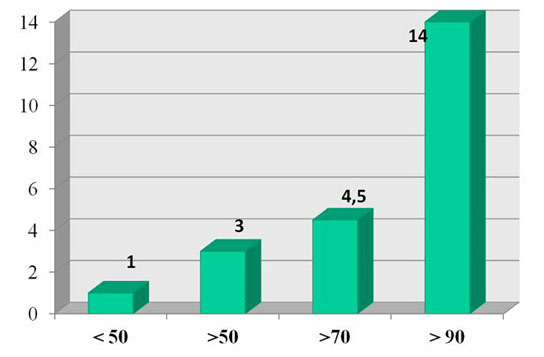
INCIDENCE OF MGUS AMONG MONOCLONAL GAMMOPATHIES
Kyle R.A.: Immunol. Rev. 194: 112, 2003
CASES: 1056 new cases of monoclonal gammopathies diagnosed in 2002 at the Mayo Clinic*
POPULATION SCREENING
· if the prevalence of the disease is >15 %
· If the disease is deadly
· if early detection of the disease reduces mortality
Principles and practice of screening for disease. WHO Public Health Papers 1968; 34.
MC detection does not require population-based screening.
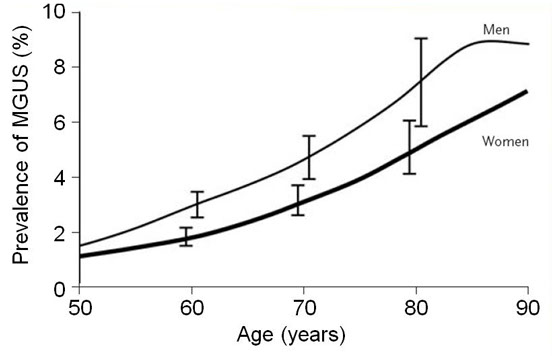
PREVALENCE STUDIES OF MGUS IN THE GENERAL POPULATION
THE PREVALENCE OF MGUS IS ELEVATED AMONG THE ELDERLY AS WELL AS AMONG MALE SUBJECTS
* Kyle R.A. et al.: NEJM 354: 1362, 2006
INCIDENCE OF MGUS ACCORDING TO AGE
Probability of progression from MGUS to MM
Prevalence of MGUS according to gender
EVOLUTION OF MGUS
Average time to malignant transformation = 10 years
1%/year ( all MGUS)
Actuarial incidence (all cases):
15% after 10 years
25% after 15 years
40% after 25 years
MGUS: RISK OF PROGRESSION
Risk of progression at 20 years from first detection:
CM <5 g/L - 14%
CM 10 g/L - 16%
CM 15 g/L - 25%
CM 20 g/L - 41%
CM 25 g/L - 49%
CM 30 g/L - 64%
Risk of developing:
MM: 25 times
MW: 46 times
Amiloydosis: 8.4 times
greater than the normal population
}
MGUS: PROGNOSTIC FACTORS FOR MALIGNANT TRANSFORMATION
At follow-up: suspect progression if
· MC concentration increases to > 3 g/dl
· MC entity is doubled (or more than doubled) compared to baseline
· upon reduction of normal polyclonal Igs
At diagnosis:
· Many studies have attempted to identify predictive prognostic factors: all agree that MGUS should be regarded as a clonal plasmacytic disease with reduced malignancy which may progress towards a symptomatic malignant lymphoid disease.
MAIN DIFFERENTIATING FEATURES OF PLASMACELLULAR
TRANSFORMATION
MGUS: PROGNOSTIC FACTORS OF MALIGNANT TRANSFORMATION
The overall aim is to discriminate between:
· low-risk MGUS
· high-risk MGUS
· Perform personalized follow-up taking into account:
· MGUS progression
· Progression with MC increase
· Steady state with sudden MC increase
MGUS progression models
PROGRESSION OF MGUS TO MYELOMA
MANY FACTORS CONCUR TO TUMOR PROGRESSION
Salmon SE: Semin Hematol, 10: 135, 1973
PATHOGENIC MODEL OF PROGRESSION FROM MGUS TO MYELOMA
INTERACTIONS OF BONE MARROW CELLS PROMOTE CLONAL PLASMACELL EXPANSION
PATHOGENIC MODEL OF PROGRESSION FROM MGUS TO MYELOMA
THE MICROENVIRONMENT OF THE BONE MARROW STIMULATES MYELOMATOUS GROWTH OF PLASMABLASTS
MGUS: PROGNOSTIC FACTORS FOR MALIGNANT TRANSFORMATION
Recent studies point to a likely situation where MGUS is characterized by serum free light chains only.
The abnormal ratio seems to indicate the early-stage of light chain multiple myeloma. In this case, patient follow-up must be performed by means of nephelometric or turbidimetric quantification of free light chains, just as in the classical case of MGUS with MC.
MONITORING MCs
Protein electrophoresis allows monoclonal component quantification. Due to the continuous risk of progression, monitoring MC concentration is thus a useful and necessary laboratory parameter.
Graziani MS, Dolci A, Greco C, Luraschi P, Muratore MT, Mussap M, Merlini G for the SIBioC protein Study Group. Indications for requesting serum protein electrophoresis BC 2008;32:48-51.
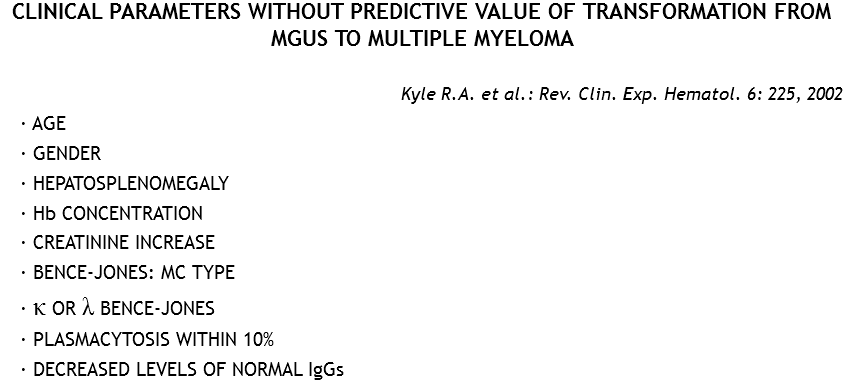
CLINICAL PARAMETERS WITH PREDICTIVE VALUE OF TRANSFORMATION FROM MGUS TO MULTIPLE MYELOMA
Kyle R.A. et al.: Rev. Clin. Exp. Hematol. 6: 225, 2002
MONOCLONAL COMPONENT
PROBABILITY OF PROGRESSION AT 20 YEARS FROM DIAGNOSIS
MGUS: unfavourable prognostic factors
· Serum M component concentration >15 g/l
· Non-IgG MGUS
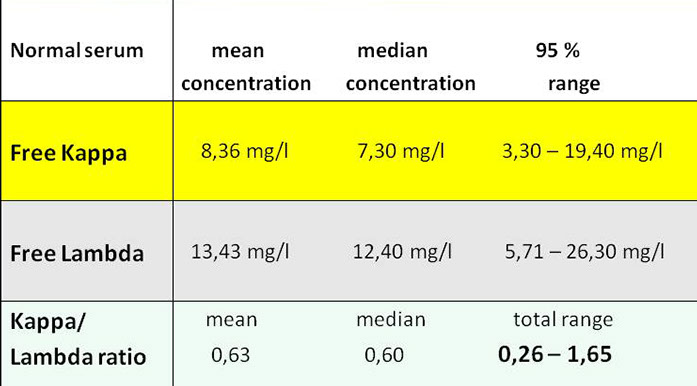
· Abnormal serum K and L free light chains ratio (FLC ratio)
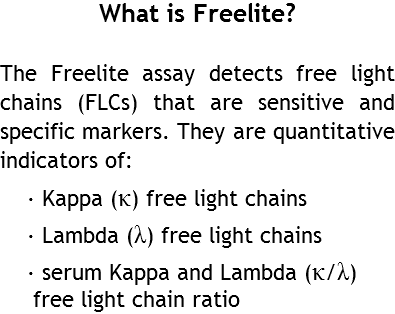
Serum FLC ratio is an indicator of monoclonality and a valuable tool for discriminating between monoclonal and polyclonal diseases.
Free Light Chains: Physiology
500-1000mg of Free Light Chain are produced per day
- 2/3 Kappa
- 1/3 Lambda
Half-life
- Kappa: 2-4 hours
- Lambda: 3-6 hours
Clearance
- Proximal tubule
- Endothelial reticular system
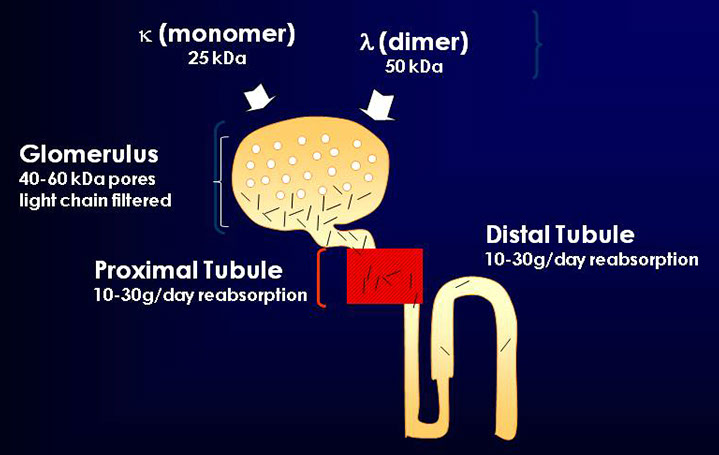
Free Light Chains: Physiology

Urine FLC
>20gm
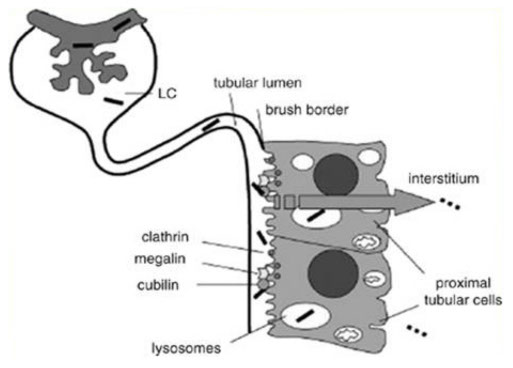
Filtration and renal reabsorbtion
λ (dimer)
50 kDa
Glomerulus
40-60 kDa pores
light chain filtered
Proximal Tubule
10-30g/day reabsorption
Distal Tubule
10-30g/day reabsorption
K/L ratio
Risk of progression: FLC ratio
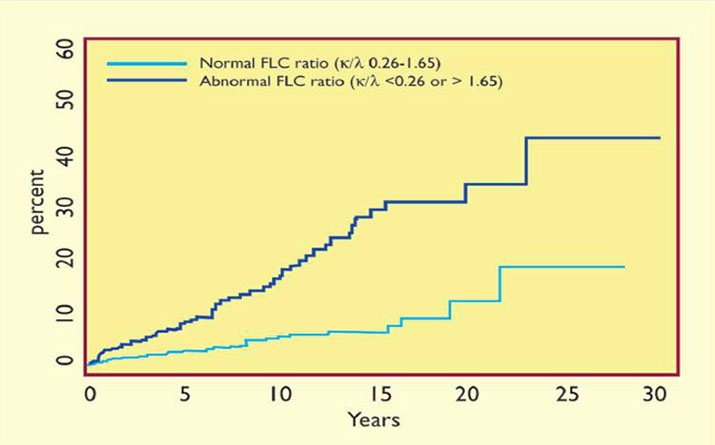
Risk of progression to MM
MGUS: summary
· During their lifetime, patients affected by MGUS are more likely to die from causes other than plasma cell dyscrasias.
· Risk for progression to frank malignancy of 1% per year
· The main indicators of progression of MGUS are: MC quantification, abnormal free light chain ratio and involved Ig type
· All patients affected by MGUS should undergo yearly check-ups
DETECTION OF THE MONOCLONAL COMPONENT
Whether incidental (in the course of routine testing) or as a result of a clinical suspect, the finding of MC implies the adhesion to conventional procedures for the detection of the latter.
Diagnostic procedure upon detection of a MC
<
>



