Monoclonal Gammopathies
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
MONOCLONAL GAMMOPATHIES
DEFINITION OF MONOCLONAL GAMMOPATHIES
· Monoclonal gammopathies are clinical-laboratoristic pictures featuring the proliferation and accumulation of B lymphocytes as well as plasmacellular clones within the bone marrow. These cells synthesize immunoglobulins (Ig) sharing identical isotypical characteristics (same Ig class) as well as idiotypical features (same antigen binding site in the variable region). They may either be complete or incomplete and can be detected in serum as well as in urine.
· Such Igs are defined as Monoclonal Components (MC)
CLASSIFICATION OF MONOCLONAL GAMMOPATHIES
NEOPLASTIC MONOCLONAL GAMMOPATHIES
· Multiple Myeloma
· Localized Plasmacytoma
· Plasma cell Leukemia
· Waldenström's Macroglobulinemia
MONOCLONAL GAMMOPATHY OF UNDETERMINED SIGNIFICANCE (MGUS)
MULTIPLE MYELOMA
· 1% of all neoplasias, 10% of all haematological malignancies among Caucasians
· The incidence increases with age and reaches its peak during the seventh decade of life.
· Predominant among males
· May be associated with exposure to toxic material, such as:
- ionizing radiation
- pesticides
- benzene
- other chemicals
· Increased risk of MM in subjects affected by MGUS (16% at 10 years)
PATHOGENIC EVENT
CLINICAL FEATURES OF MM
· 30% of cases are diagnosed incidentally, in the course of routine examinations
· Clinical features characterize the remaining 70% of cases
· The most common clinical presentations are the following:
- Skeletal affections: due to cytokine production
- Renal failure: due to increased excretion of free light chains in the urine (Bence-Jones Proteinuria)
- Infectious morbidities: due to immunosuppression
SKELETAL AFFECTIONS
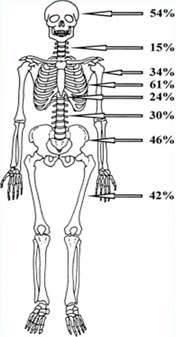
· 70% of patients present such affections at diagnosis. Almost all patients present such symptoms at relapse
· It may affect any bone (mainly spine and flat bones) responsible for myelopoiesis
· Osteolytic lesions, osteoporosis and mixed clinical features
· It greatly affects the patient's quality of life (pain, risk of complications such as pathological fractures, vertebral collapse, spinal cord compression)
· Possibility of developing extraosseous affections
Pathogenesis of bone diseases in MM
Ostelytic lesions in MM are caused by:
· Increased bone resorbtion due to increased osteclast activity
· Reduced bone formation due to diminished osteoblast activity
Bone remodeling
SKELETAL XR SURVEY
· Detects alterations in 60-70% of patients
· Circumscribed osteolysis in the absence of periosteal sclerosis, osteopenia or mixed clinical presentations
· Detects lesion only upon 50% reduction of bone mass
· Possible underestimation of injuries due to misdetection of small lesions as well as low resolving power in the vertebral region

Osteoporotic bone
pattern

Patterns
of osteolysis
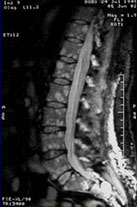
NUCLEAR MAGNETIC RESONANCE
· Qualitative evaluation of bone marrow: typical T1-hypointense lesions, T2- hyperintense lesions, strong uptake of the contrast agent (gadolinium)
· Patterns of alterations: Focal, variegate, diffused patterns
· High resolving power in the vertebral region. Discriminates between disease/osteoporosis and identifies any neurological complications
· Evaluation of extraosseous masses
· Limited visual field

Normal
pattern
Focal
pattern

Diffused
pattern
RENAL FAILURE
· Affects approximately 50% of patients
· Initial symptom in 10-20% of cases. In the remaining subjects, it appears as the disease progresses.
· Multifactorial pathogenesis:
- Bence-Jones proteinuria
- Hypercalcemia
- Nephrotoxic substances: FANS, antibiotics, iodinated contrast media
- Infections/dehydration
· Other histopathological presentations
RENAL FAILURE
Histopathological and functional pictures
HYPERCALCEMIA SYNDROME
· Affects approximately 30-40% of MM patients, half of which upon onset, whereas the other half during disease progression
· Pathogenetically due to increased bone resorption and consequent calcium release in the blood stream
· Clinical manifestations: polyuria, polydipsia, anorexia, nausea, vomiting, asthenia. If the symptoms persist: dehydration, confusion, delirium and coma (hypercalcaemic encephalopathy)
INFECTIOUS MORBIDITY
· Humoral immune deficiency
· Increased incidence of infectious diseases (mainly due to bacterial infections)
· Uncommon at onset although it progressively becomes more significant during the clinical course (disease recurrence and therapy-induced immunosuppression)
Infections are the leading cause of death among MM affected patients
Bone marrow failure: multifactorial "secondary" anemia
· Bone marrow invasion
· Erythropoietin deficiency
- Chronic Kidney Disease (CKD)
- Inadequate production
· Drug-induced myelosuppression
· Production of inflammatory cytokines
APPROACH TO PATIENTS WITH SUSPECTED MYELOMA
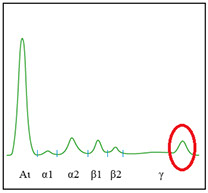
LABORATORY INVESTIGATIONS (I)
· Total proteinemia + electrophoresis (hyper- or hypogammaglobulinemia)
· Ig quantification
· 24 hour proteinuria: quantification of urinary monoclonal free light chain excretion
· Characterization of the MC (by means of serum and urine immunofixation)
· Quantification of serum free light chains

APPROACH TO PATIENTS WITH SUSPECTED MYELOMA
LABORATORY INVESTIGATIONS (II)
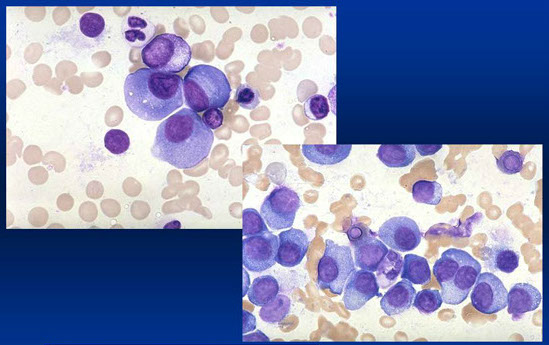
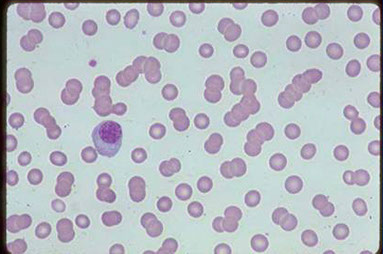
· Bone marrow aspirate
· Bone biopsy
· Karyotype and molecular analysis of alterations of plasma cells
MM bone marrow aspirate
APPROACH TO PATIENTS WITH SUSPECTED MYELOMA
INSTRUMENTAL INVESTIGATIONS: IMAGING TECHNIQUES
· Total XR surveys (skull, shoulders, ribs, spine, pelvis, femurs)
· NMR
· CAT, 18F-FDG-PET/TC, scintigraphy with 99mTechnetium Sestamibi
Fundamental for correct staging
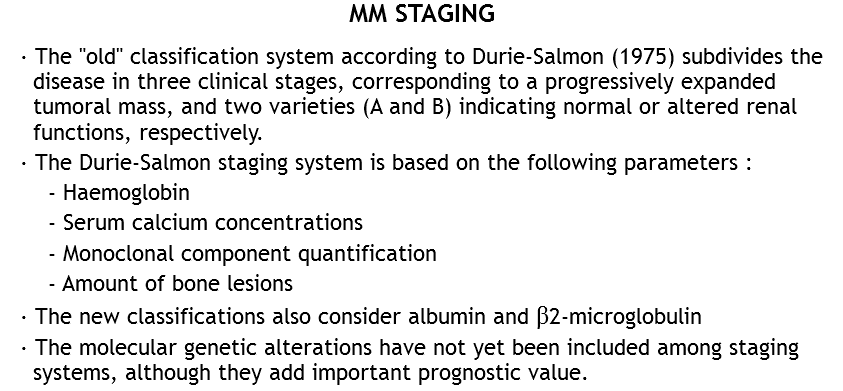

PROGNOSTIC FACTORS
CYTOGENETIC ALTERATIONS
· Monosomy or deletion of chromosome 13
· Ig heavy chain gene translocations of the 14q32 locus (especially t(4;14) and (6;14))
· Deletion of chromosome 17 (anti-oncogene P53)
· Amplification of the CKS1B gene located on chromosome 1
THERAPEUTIC STRATEGIES
When should therapy be initiated?
· Therapy should be administered upon appearance of MM symptoms, that is, in the presence of organ damage
CRITERIA OF DISEASE ACTIVITY IN MM (CRAB)
· C : HYPERCALCAEMIA (Ca++ ≥ 11.5 g/dL)
· R : RENAL INSUFFICIENCY (CREA > 1,73 mmol/L)
· A : ANEMIA (Hb over 2g below normal values or <10 g/dL)
· B : BONE LESIONS (lytic lesions, osteopenia, pathologic fractures)
THERAPEUTIC STRATEGIES
· Therapy should be administered according to age
· Elderly patients > 65 years: chemotherapy at conventional doses with the addition of new drugs directed against the bone marrow microenvironment
· Young patients < 65 years: high dose chemotherapy as well as hematopoietic progenitor cells (autologous or allogeneic) transplant. Possible addition of new drugs directed against the bone marrow microenvironment
MONOCLONAL GAMMOPATHY OF UNDETERMINED SIGNIFICANCE (MGUS)
· Incidentally diagnosed in the course of other laboratory investigations
· Absence of clinical manifestations (no symptoms or organ damage)
· Incidence increases with age
· Does not require therapy
INCIDENCE OF MGUS ACCORDING TO AGE
MGUS: DIAGNOSTIC CRITERIA
· Monoclonal component concentration ≤30 g/dL
· Bone marrow plasma cell infiltration ≤10%
· Normal concentrations of the remaining immunoglobulin classes
DIFFERENTIAL DIAGNOSIS:
MGUS/1st STAGE MM /SYMPTOMATIC MM
PROBABILITY OF PROGRESSION AMONG 1384 PATIENTS AFFECTED BY MGUS
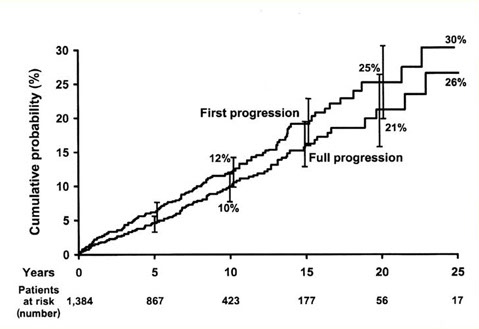
Kyle RA, NEJM 2002
WALDENSTRÖM'S DISEASE
MONOCLONAL NEOPLASTIC DISEASE AFFECTING B CELLS OF THE LYMPHOID SYSTEM, CHARACTERIZED BY THE PROLIFERATION AS WELL AS THE ACCUMULATION OF LYMPHOPLASMOCITOID ELEMENTS PRODUCING STRUCTURALLY HOMOGENEOUS IgM-TYPE Igs
WALDENSTRÖM'S MACROGLOBULINEMIA
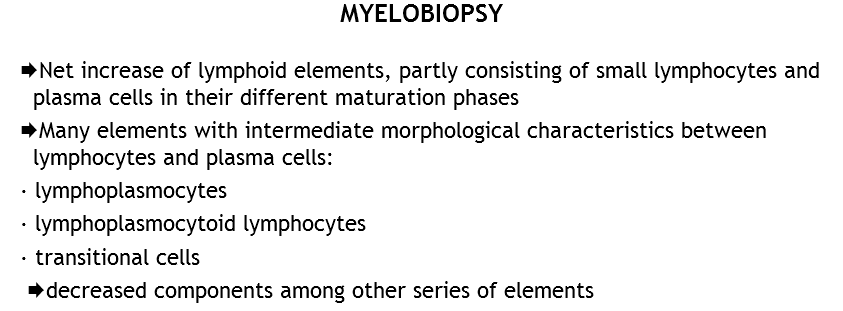
· Characterized by infiltration of bone marrow by mature lymphocytes, plasmocytoid lymphocytes and plasma cells
· Affects elderly adults (median age: 63 years)
· The diagnosis can be incidental, leading to the finding of increased IgM concentrations
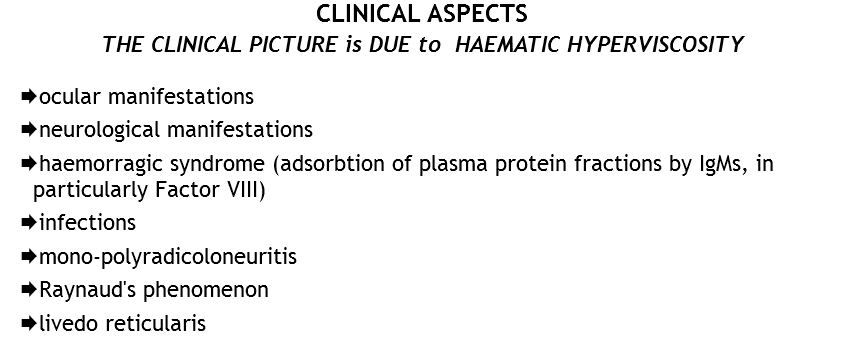
· The clinical pictures are characterized by:
- Hyperviscosity syndrome
- Anemia or cytopenias: due to bone marrow infiltration
- Lymphadenomegaly-hepatosplenomegaly
- Peripheral polyneuropathy: due to the anti-myelin antibody activity of the M-component
EPIDEMIOLOGY
RARE DISEASE, MAINLY AFFECTING THE ELDERLY, UNDISTINCTIVE OF AGE OR GENDER
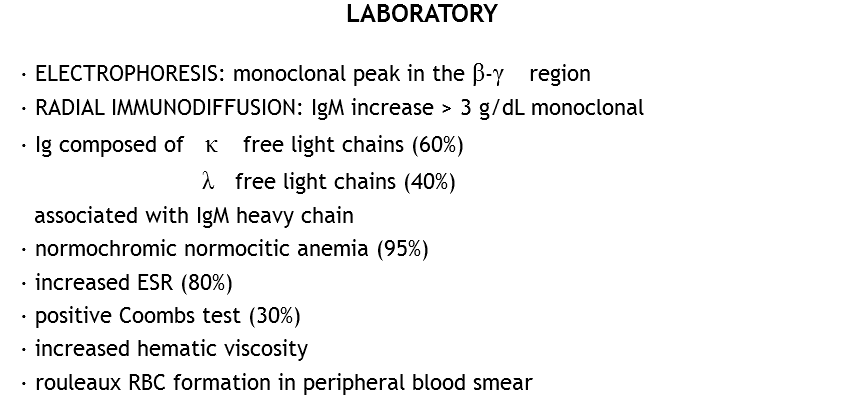
Hyperviscosity syndrome
· Usually breaks out at IgM concentration levels > 3 g/dL
· Affects sight (visus reduction, retinic haemorragias)
· Neurological affections (headache, ear buzzing, concentration and memory problems, somnolence and coma)
· Bleeding diathesis due to thrombocytopenia and coagulation factors deficiency
· Treatment of election: plasmapheresis
Neurological manifestations
· Predominantly characterized by sensory peripheral polyneuropathy, with a progressive course
· Mainly associated to IgA or IgM
· 50% of cases show anti-MAG activity
· Can be associated to MGUS
· Can be worsened by the use of drugs
Prognosis and progression
· median survival: 5 years
· lack of clinical response to treatment: adverse prognostic factor
<
>



