IgD Myeloma
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
IgD myeloma
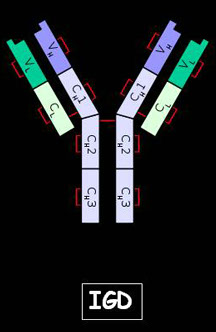
IgD immunoglobulins
· IgDs (M.W.= 175.000 Daltons) display monomeric structures. They may essentially operate during fetal development.
· They may play a role in the development of the immunological memory or they may simply represent an evolutionary legacy.
LIQUID PHASE QUANTIFICATION
NEPHELOMETRY: the antigen reacts with a highly specific antibody. An antigen-specific antibody complex is formed, even in the presence of other proteins.
The light beam of the nephelometer is deflected (scatter).
The higher the protein concentration, the more numerous and larger the complexes, and thus the greater the deviation.
Nephelometric quantification of IgDs
· The nephelometric quantification of IgDs as well as of all low concentration proteins requires great attention. In the presence of of strong antigen excess, the signal underestimates protein concentration, thus distorting the results.
· Performing a pre-reaction excludes the possibility of false negative results.
· Pre-reactions enable the evaluation of significant signal increases. This is achieved by mixing an aliquot of the sample with the total amount of antiserum. Upon signal increases beyond a predefined threshold, the assay is automatically rerun at higher dilutions.
· New dilutions also undergo repeated pre-reaction processes until the signal reaches specific threshold values. The latter are automatically calculated by the instrument, by means of mathematical algorithms.

IgD quantification in MM
· Quantitative assay systems employ antisera that are unable to discriminate between monoclonal and polyclonal immunoglobulins.
· The calibrator relies on a polyclonal antigen, which is therefore much different from the monoclonal antibody in the sample. The assay thus lacks the essential requirement for immunoassay accuracy, that is, the parallelism between the calibrator and the analyte.
· Despite criticisms, quantitative IgD measurement is nonetheless performed, as it conveys further information to clinicians concerning the activity of clonal cells.
Graziani MS et al.per il GdS Proteine SIBioC.
Indications for requesting serum protein electrophoresis BC 2008;32:48-51.
MONOCLONAL GAMMOPATHIES
MGs comprise a variety of clinical conditions, ascribed to three different causal mechanisms:
1. disease variants exhibiting clinical manifestations due to the proliferation of neoplastic clones
2. disease variants exhibiting clinical manifestations due to pathological effects of MC
3. clinically occult disease variants.
Serum protein electrophoresis (EF) in the case of IgD myeloma may yield the following patterns:
· A minimally detectable M protein peak, usually in the beta-gamma region.
· A large percentage of cases show hypogammaglobulinemia or a normal serum electrophoretic pattern
Shimamoto Y.. Cancer Detection e Prevention, 19 (5): 426-435, 1995.
Typing the monoclonal component
Analytical technique: serum or urine protein Immunofixation (considered the gold-standard for detecting MCs),
IMMUNOFIXATION (IFE)
SEPARATION PHASE
SOLID-PHASE ELECTROPHORESIS
+
anti-
γ α μ δ ε κ λ chains antisera
IMMUNOLOGICAL PHASE
Sensibility: 0.005 g/L
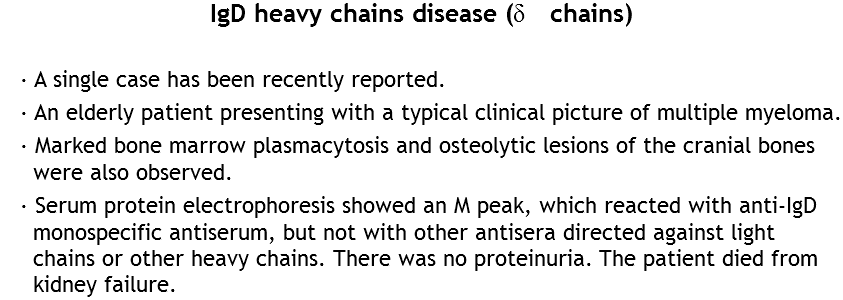
Two clinical cases of IgD-myeloma
· IgD myeloma is characterized by an IgD MC almost always associated with a prevalence of Lambda light chains, along with Bence-Jones proteinuria and renal failure.
· IgD displays a very short biological half-life in peripheral blood, with a 26% catabolic rate reaction per day. As IgD MCs show poor statistical incidence, their routine laboratory immunochemical investigations are often underestimated.
Two clinical cases of IgD myeloma
· IgD paraproteins have higher catabolic rates compared to IgGs, IgAs and IgMs, but lower rates compared to IgEs.
· Indeed, the IgD molecule has long hinge regions between the Fab and Fc fragments, which make them more susceptible to proteolytic degradation.
· Due to this rapid catabolism in serum, IgD detection in urine is very rare.
· Thus, in 90% of cases, only light chains are detected in the urine, accounting for most proteinuria
Mercks index 2010
Clinical Case no. 1
· A 50 year old woman presented to our ambulatory care center with a previous history of lambda light chain multiple myeloma
· Her complete blood cell count was within normal range values;
serum Ca concentration of 10.5 mg/dL was within normal range values (n.v.) 8,5-10,5 mg/dL.
· Serum protein electrophoresis showed low gamma globulin percentages 9.7% (n.v. 11,1-18,8) with a serum protein concentration of 6.8 g/dL (n.v. 6,5-8,5 g/dL).
· The suppression of all immunoglobulin classes was reported, with the following Ig values: IgG,302(n.v. 800-1600 mg/dL) IgA 22.1( n.v.70- 400 mg/dL) and IgM 19 (n.v. 40-230 mg/dL)
· Bence-Jones proteinuria was carried out following a positive initial screening by means of urine penta IFE.
· Serum IgD and IgE quantification yielded the following results: 1602 ( n.v. 0-100 mg/dL) as well as 60 (n.v. less than 100 mg/dL).
Clinical Case no. 1
The initial diagnosis of light chain multiple myeloma was confirmed upon performance of the first serum and urine IFEs.
Nevertheless, the EF patterns showed bands located in positions that are typical of heavy chain monoclonal components.
This led us to carry out further serum tests using anti-IgD and IgE antisera.

Clinical Case no. 1
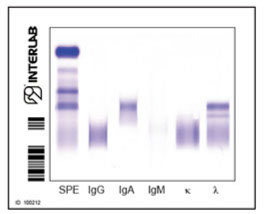
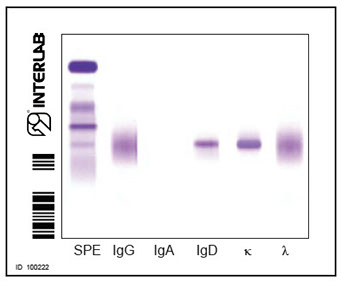
· Serum IFE of the patient showed the presence of an IgD kappa monoclonal component, with kappa light chains being a very rare finding among this kind of plasma cell dyscrasias.
Clinical Case no. 2
· The second patient was a woman aged 57. She underwent physical examination following immunofixation tests, indicative of an undefined form of myeloma.
· The total blood count was within range, with serum calcium levels of 12,2 mg/dL. Serum protein electrophoresis showed 10% gamma globulins and 7,2 g/dL of serum protein concentration.
· Suppression of IgGs, IgAs and IgMs was also observed, and their respective concentrations were as follows: 500mg/dL; 60 mg/dL; 30 mg/dL.
· The Bence-Jones screening test was also positive.
· Serum IgE concentration amounted to 870 mg/dL whereas serum IgE concentration was 52mg/dL.
Clinical Case no. 2
· The immunochemical pattern of this patient was rather complex, showing a double lambda band, possibly due to the heavy chain as well as to the presence of Bence-Jones protein.
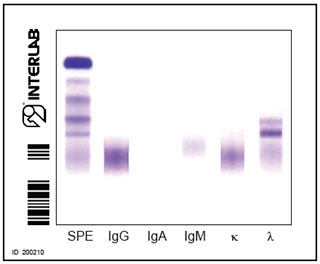
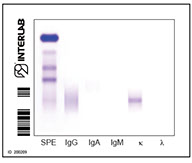
Two monoclonal λ bands detectable by means of serum IFE
Clinical Case no. 2
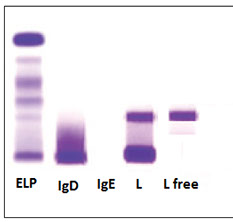
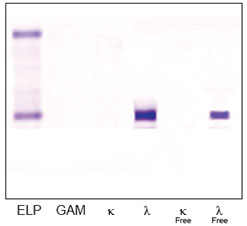
The immunochemical pattern shows the presence of an IgD lambda monoclonal component, along with monoclonal free Lambda light chains in both serum and urine
<
>



